


Definition of terms related to normal labour:
LABOUR:
is described as the process by which the fetus, placenta and membranes are expelled through the birth canal.
LIGHTENING:
2-3 weeks before the onset of labour,the lower uterine segment expands and allows fetal head to sink lower, it may engage.
The fundus no longer crowds the lungs, thus breathing is easier, the heart and stomach can function more easily and the woman experiences relief which is known lightening
ATTITUDE:
This refers to the posturing of the joints and relation of fetal parts to one another.The normal fetal attitude when labor begins is with all joints in flexion.
?Fetal Orientation
1.Fetal lie
2.Fetal presentation
3.Fetal position
1.Fetal lie
Refers to the relationship of the long axis of the fetus to the long axis of the mother
Longitudinal: 99% of all fetuses assume this lie.
Transverse: long axis of the fetus is perpendicular to the long axis of the mother.
Result of over-relaxation of maternal abdominal wall
Increased risk with multiple pregnancies
Requires a C-section
Oblique: the relationship of the spines forms <45 degree angle.
-Fetal lie include;
- Longitudinal
- Transverse
- Oblique
2.Fetal presentation
Presenting part,
Refers to the part of the fetus that enters the canal first
This include;
- Cephalic- Vertex: head with chin flexed toward chest (most common cephalic see position)
- Face: fetus’s neck is hyper-extended bringing the back of its head
- Breech
- Shoulder
?THE CAUSE OF THE ONSET OF LABOR:
1. HORMONAL FACTORS
Release of oxytocin
Altered Estrogen, progesterone ratio.
2.BIOCHEMICAL FACTORS
Prostaglandin.
3.MECHANICAL FACTORS:
Formation of fore water.
General fluid pressure.
Pressure from the presenting part.
Over stretched uterus.
Rupture of the membrane.
Fetal axis pressure.
Recognition of first stage of labour:
-Presence of blood show
-Contractions =(Braxton hicks) contractions.
Painful rhythmic regular contractions.
-Rupture of membranes.
-Cervix dilatation as confirmed by midwife.
➡️ THE DIFFERENCE BETWEEN TRUE LABOR AND FALSE LABOR
Differentiation between the true and false labour
(A) FALSE LABOUR: (false or spurious):
- Begin and remain irregular
- Felt first abdominally and remain confined to the abdomen, often disappear with ambulation.
- Do not increase in duration, frequency or intensity.
- No retraction or dilatation of the cervix.
(B) TRUE LABOR/CONTRACTIONS:
- Begin irregularly but become regular and predictable
- Felt first in lower back and sweep around to the abdomen
- In a wave Continue no matter what the women’s level of activity
- Increase in duration, frequency and intensity.
- Achieve cervical dilatation.
True labour:
Labour is said to be established with regular rhythmic painful contractions.uterine contraction occurs and effacement of cervix with 2cm dilated.
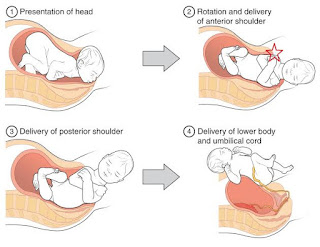
? MECHANISM OF NORMAL LABOR
? STAGES OF NORMAL LABOUR:
IT HAS FOUR STAGES. These stages are described as:
1. The first stage of labour :
It begins with painful regular rhythmic contraction and is complete when the cervix is fully dilated.
2. The second stage of labour:
It begins when the cervix is fully dilated and is completed when the baby is completely born.
3.The third stage of labour: It begins with the delivery of the baby and ends with complete expulsion of placenta and membranes. It also involves the control of bleeding.
4. 4TH Stage of labour:
Starts from complete expulsion of the placenta and membrane and ends at 1hour after delivery.
Physiology of the first stage of labour:
Duration :
It varies but influenced by parity, birth interval, psychological state, presentation and position, pelvic shape and its size, character of uterine contractions.
Great part of labour is taken by first stage of labour, and active labour to be completed within 12 hrs, for primgravida and multipara to be 6hrs to reach second stage
Uterine action:
Usually did happen by the aid of the following activities:
1) Fundal dominance:
Each uterine contraction starts in the fundus near one of the cornua and spreads across and downwards. The contraction lasts longer in the fundus where it also more intense but the peak is reached simultaneously over the whole uterus and the contractions fades from all parts together .
This process enables the cervix to dilate and the strongly contracting fundus to expel the fetus.
2) Polarity:
Is the neuromuscular harmony that prevails between the two poles or segments of the uterus throughout labour.
During each contraction these two poles act harmoniously.The upper part pole contracts strongly and retracts to expel the fetus. The lower pole contracts slightly and dilates to allow expulsion to take place.
If polarity is disorganized,the progress of labour is inhibited.
3) Contraction and retraction:The process of shortening and relaxation of muscle fibers of the uterus.
Assist in the progressive expulsion of the fetus, where by the upper segment of uterus becomes gradually shorter and thicker and its cavity diminishes.
early labour contractions occurs every 15-20 minutes, lasts for 30 seconds.
Usually weak and mother can accept and tolerate. End of first stage : occur 2-3 minute interval, last for 50-60seconds and are very powerful.
Formation of the upper and lower uterine segments:
At full term the body of uterus has divided
itself in to two which are anatomically distinct.
-Upper part = mainly concern for contractions and is thick and muscular,
-Lower part= is prepared for distension and dilatation of cervix and is thinner.
-The lower segment develops from isthmus, and is 8-10 cm in length.
During labour the retracted longitudinal fibers in the upper segment pull on the lower segment causing it to stretch aided by descending head or breech.
5)The retraction ring:A ridge forms between the upper and lower uterine segments which is known as the retraction or( bandls ring).
The normal retraction ring rises as the upper uterine segment contracts and retracts and thins out to accommodate the descending fetus.
6) Cervical effacement:
If the cervix has not already been taken up during the last days of pregnancy, this process will take place in labour.
The muscle fibers surrounding the internal os are drawn upwards by the retracted upper segment and the cervix merges into the lower uterine segment.
7) Cervical dilatation:
Dilatation of the cervix is the process of enlargement of the external os from a tightly closed aperture to an opening large enough to permit passage of the fetal head.
-Measured in cm fully is 10cm.
8) show:
-Due to dilatation of cervix the operculum which formed the cervical plug during pregnancy, is lost.
There will be a blood stained mucoid discharge a few hours before or within few hours after labour start
☑️ Phases of the First Stage of normal Labour
-The painful contractions increase in frequency, intensity, duration and force as labor advances.
-The cervix also dilates simultaneously from
0 -10 cms (full dilation) at the end of the first stage of labour.
1.Phase I or the Latent Phase of Labor:
-Uterine contractions is very mild .
-They are irregular and not forceful enough to cause much pressure on the cervix.
-The cervix slowly becomes shorter and softer. This is known as ‘Effacement’.
-Dilation of the cervix occurs from 0 – 4 cm.
-The frequency of the uterine contractions at this stage is from 1-3 per 10 minutes in normal labour and each contraction lasts for less than a minute.
-The uterus may become firm and more prominent with every contraction.
In some women, the labor pains start at the back.This is more likely if the head of the fetus is more posteriorly placed and presses on the mother’s spine or ligaments.
2.Phase II or the Active Phase of labor:
-This is the phase where the uterus contracts more frequently and the pain is maximum.
-Uterine contraction occurs after every 3-5 minutes and lasts for more than a minute.
-The uterus becomes hard and more prominent as the pain increases and softer as the uterus relaxes.
-The pains sometimes start at the back and radiates down to the thighs.
-Later on, at the end of this stage, the pains come even more frequently and appear to run into each other in quick succession.
-The cervix dilates from 4 cm to 8 cm.
-Women whose waters have not ruptured at the onset of labour, can experience a gush of water flowing out of the vagina at this stage.
3. Phase III or the Transitional Phase of Labor:
This phase is called the transitional phase because it marks the transition from the first stage of labour to the second stage of labour. The cervix dilates from 8 – 10 cm.
-At full dilatation at the end of the first stage of labour, the cervix is about 10 cm (4 inches) in diameter.
– Since the maximum diameter of the fetal head is also 10 cm when it is in a normal position, the baby can be born easily through the cervix.
? management of first stage of normal labour
-The principle of management of this stage is to prepare the patient to have a safe vaginal delivery and to carefully monitor the vital signs for early detection of any deviation from the normal.
Cont:management:
Thorough general and obstetrical examination is done as soon as labor pains start to plan for an uncomplicated labour, to check for a normal fetal heart rate and to exclude any cephalopelvic disproportion (where the diameter of the head is larger than the mother’s pelvis).
Is the care given throughout the 1st stage of labour.
Admission procedure:
Well coming the mother and her partner
On Arrival – Greet the mother
– Introduce your self
– Inform relative to wait
-Check- show rupture of membrane
regular uterine contraction with progressive cervical dilatation
History:
Information from the mother
-Ask the mother onset of contraction
Rupture of membranes / passage of liquor
Show or any other bright red bleeding.
Physical examination:
The general condition
Exhausted, anemic, pain, dehydrated general edema
Vital sign: Blood Pressure, Temperature, pulse, respiration
Cont: management:
Abdominal examination:
Inspection: size, shape, previous scar.
Palpation: lie, présentation, attitude, engagement and contractions.
Fundal height.
Auscultation fetal heart rate & rhythm
Cont: management:
Vaginal examination:(Indications)
-To make a positive diagnosis of labour
-To exclude cord presentation or cord prolapsed after rupture of membrane.
cervical dilatation









How can I download the notes
Kitabu kizuri kujikumbushia
Sante sana for feedback